1. Introduction
Femoroacetabular Impingement Syndrome (FAIS) is a condition resulting from abnormal contact between the femoral head and the acetabulum, leading to hip pain and movement restrictions. This occurs due to morphological changes, including cam and pincer deformities, which contribute to joint damage and functional impairment. The resulting mechanical stress can provoke synovial inflammation, cartilage degradation, and pain exacerbation, significantly impacting mobility and quality of life [
1,
2,
3,
4,
5]. Over the past two decades, FAIS has gained increasing attention from the scientific community, with a growing body of research focused on its pathophysiology, diagnostic tools, and treatment approaches [
6,
7,
8,
9,
10,
11,
12]. Despite advancements in diagnostic imaging and rehabilitation approaches, the effectiveness of conservative treatment remains inadequately defined. Traditionally, surgical intervention—especially hip arthroscopy—has been considered the primary treatment for FAIS, with the aim of correcting morphological abnormalities and alleviating symptoms [
1,
6,
13,
14,
15]. Several studies have reported significant improvements in pain relief, return to activity, and overall patient satisfaction following surgery [
16,
17,
18,
19,
20,
21,
22]. However, surgical procedures are not without risks, including post-operative complications, persistent pain, and long-term joint degeneration [
23,
24,
25,
26]. Consequently, conservative treatment options have emerged as viable alternatives, aiming to delay or even prevent the need for surgery while improving functional outcomes. Physiotherapy-based interventions, including motor control training, muscle strengthening, manual therapy, and patient education, have been explored as potential non-invasive strategies for managing FAIS [
27,
28,
29,
30,
31,
32,
33]. Recent systematic reviews have examined various rehabilitation approaches, suggesting that targeted exercise therapy, particularly core stability training and hip muscle strengthening, may enhance functional performance and alleviate symptoms. The heterogeneity in treatment protocols for FAIS reflects the multifactorial nature of the condition, emphasizing the need for standardized rehabilitation guidelines [
3,
4,
34,
35,
36,
37,
38]. Additionally, there is a lack of consensus on the optimal rehabilitation strategies, making it difficult to establish definitive clinical guidelines. One of the primary limitations in the current literature is the inconsistent diagnostic criteria used to identify FAIS across studies. Imaging plays a key role in identifying bony abnormalities associated with FAIS, such as cam and pincer lesions. However, structural findings alone do not always correlate with symptom severity, highlighting the importance of a comprehensive clinical assessment. Moreover, previous systematic reviews have either focused exclusively on surgical versus conservative management or have included a broad range of hip disorders, limiting the specificity of their conclusions regarding FAIS rehabilitation [
39,
40,
41,
42,
43,
44]. This scoping review aims to identify and evaluate physiotherapy interventions for FAIS, analyzing their effectiveness in pain reduction, functional improvement, and quality-of-life enhancement. By synthesizing the most recent evidence on pain management, functional improvement, and quality-of-life outcomes, this review will provide a comprehensive assessment of the effectiveness of physiotherapy-based treatments. The ultimate objective is to establish whether conservative rehabilitation can serve as a viable first-line treatment for FAIS, offering an evidence-based alternative to surgery and informing clinical practice on best rehabilitation strategies.
2. Methods
The present scoping review was conducted following the methodological framework outlined by the Joanna Briggs Institute (JBI) [
45], which provides structured guidance for scoping reviews. To ensure methodological rigor and transparency, the review process adhered to the PRISMA Extension for Scoping Reviews (PRISMA-ScR) guidelines [
46].
2.1. Review Question
We formulated the following research question: What is the effectiveness of evidence-based conservative treatment approaches in patients diagnosed with Femoroacetabular Impingement Syndrome?
2.2. Eligibility Criteria
Studies were eligible for inclusion if they met the following Population, Concept, and Context (PCC) criteria.
Population (P): The Population criterion included patients diagnosed with Femoroacetabular Impingement Syndrome (FAIS), a musculoskeletal disorder characterized by abnormal contact between the femoral head and the acetabulum, leading to pain, reduced range of motion, and functional impairment. Studies were eligible if they included patients diagnosed based on clinical assessment and/or imaging findings such as radiography, MRI, or CT scans. The age range considered was 16 years and older, as FAIS primarily affects young and middle-aged adults. Patients with significant comorbidities, including oncological, rheumatological, or neurological conditions that could interfere with rehabilitation outcomes, were excluded. Pediatric populations under 16 years of age were also not considered. Additionally, studies without full-text availability were excluded from the review, as their content could not be critically assessed.
Concept (C): The Concept criterion focused on conservative physiotherapeutic interventions for FAIS management. Studies were considered if they examined rehabilitation strategies, including exercise therapy, manual therapy, education-based interventions, or multimodal rehabilitation programs. Exercise therapy included strengthening programs targeting hip and core muscles, neuromuscular training, flexibility exercises, and motor control interventions. Manual therapy encompassed joint mobilization, soft tissue techniques, and myofascial release, while education-based interventions involved patient education on activity modification, posture correction, and self-management strategies. Multimodal rehabilitation programs combining different therapeutic approaches were also considered. Studies were excluded if they focused solely on surgical interventions or compared different surgical techniques without incorporating conservative treatment. Additionally, research that did not specify physiotherapy-based treatments or lacked a structured rehabilitation protocol was not included.
Context (C): The Context criterion focused on clinical settings where conservative management of FAIS was applied. Eligible studies were those conducted in outpatient rehabilitation centers, hospitals, sports medicine clinics, or research institutions where physiotherapy interventions were implemented for FAIS patients. Studies that took place in primary care settings or general orthopedic clinics were included if they provided structured rehabilitation programs delivered by physiotherapists or rehabilitation specialists. The review excluded studies conducted in exclusively surgical settings or those that did not involve a physiotherapy-based rehabilitation approach. Contextual variability across different healthcare systems and patient populations was considered to ensure that findings were generalizable to diverse clinical environments.
Although the eligibility criteria did not explicitly limit the selection to Randomized Controlled Trials (RCTs), the methodological rigor and inclusion criteria focusing on comparative studies led to the exclusive selection of RCTs.
2.3. Exclusion Criteria
Studies that did not align with the defined Population, Concept, and Context (PCC) criteria were excluded to maintain the review’s focus and relevance to its objectives.
2.4. Search Strategy
A structured and systematic search was initially performed in MEDLINE via PubMed to identify relevant studies. The keywords and controlled vocabulary terms retrieved from the preliminary search results were then refined to develop a comprehensive search strategy. This refined strategy was subsequently adapted and applied across multiple databases, including the Cochrane Central Register of Controlled Trials (CENTRAL), Scopus, PEDro, and Web of Science, ensuring the broad coverage of the available literature. The database searches were completed on 23 January 2024, without restrictions on the publication date. The search strategy was adapted for each database to maximize relevant findings, prioritizing controlled vocabulary terms where applicable (e.g., MeSH terms in PubMed) and using keyword searches in databases without indexed subject headings. Below are the detailed search strategies tailored for each database:
MEDLINE(PubMed):
(“Femoroacetabular Impingement Syndrome” [MeSH] OR “Femoroacetabular Impingement” OR “Hip Impingement” OR “FAI Syndrome” OR “FAI” OR “Femoroacetabular impingement syndrome” [TIAB])AND (“Physical Therapy Modalities” [MeSH] OR “Rehabilitation” [MeSH] OR “Physiotherapy” OR “Physical Therapy” OR “Exercise Therapy” [MeSH] OR “Therapeutic Exercise” OR “Manual Therapy” [MeSH] OR “Core Stability” OR “Motor Control Training” OR “Neuromuscular Training”) AND (“Conservative Treatment” OR “Non-Surgical Management” OR “Non-Operative Treatment” OR “Rehabilitation Protocol” OR “Evidence-Based Rehabilitation” OR “Non-Surgical Intervention” OR “Exercise-Based Therapy”) NOT(“Total Hip Arthroplasty” [MeSH] OR “Hip Replacement” OR “Surgical Procedure” OR “Case Reports” [Publication Type])
Cochrane Central:
(femoroacetabular impingement OR FAI OR hip impingement OR femoroacetabular impingement syndrome) AND (physical therapy OR physiotherapy OR rehabilitation OR exercise therapy OR manual therapy OR therapeutic exercise OR motor control training OR core stability OR neuromuscular training) AND (conservative treatment OR non-surgical management OR rehabilitation protocol OR non-operative treatment OR evidence-based rehabilitation OR non-surgical intervention) NOT (arthroplasty OR hip surgery OR total hip replacement OR case reports)
Scopus:
TITLE-ABS-KEY (“Femoroacetabular Impingement” OR “FAI Syndrome” OR “Hip Impingement” OR “Femoroacetabular impingement syndrome”) AND TITLE-ABS-KEY (“Physiotherapy” OR “Rehabilitation” OR “Physical Therapy” OR “Exercise Therapy” OR “Manual Therapy” OR “Therapeutic Exercise” OR “Core Stability” OR “Neuromuscular Training” OR “Motor Control Training”) AND TITLE-ABS-KEY (“Conservative Treatment” OR “Non-Surgical Management” OR “Non-Operative Treatment” OR “Rehabilitation Protocol” OR “Evidence-Based Rehabilitation” OR “Exercise-Based Therapy”)
PEDro:
(femoroacetabular impingement OR hip impingement OR FAI syndrome) AND (physiotherapy OR physical therapy OR rehabilitation OR manual therapy OR therapeutic exercise OR exercise therapy OR core stability OR neuromuscular training OR motor control) AND (conservative treatment OR non-surgical management OR non-operative treatment OR rehabilitation protocol OR evidence-based rehabilitation OR functional training) NOT (surgery OR arthroplasty OR total hip replacement OR surgical intervention)
Web of Science:
TOPIC: (“Femoroacetabular Impingement” OR “FAI Syndrome” OR “Hip Impingement” OR “Femoroacetabular impingement syndrome”) AND TOPIC: (“Physiotherapy” OR “Rehabilitation” OR “Physical Therapy” OR “Exercise Therapy” OR “Manual Therapy” OR “Core Stability” OR “Neuromuscular Training” OR “Motor Control Training”) AND TOPIC: (“Conservative Treatment” OR “Non-Surgical Management” OR “Rehabilitation Program” OR “Evidence-Based Rehabilitation” OR “Exercise-Based Therapy”)
2.5. Study Selection
The study selection process was carried out in a structured and systematic manner, adhering to the standards for scoping reviews. All search results were compiled, and duplicate records were eliminated using Zotero. The screening procedure was conducted in two sequential phases: an initial review of titles and abstracts to identify potentially relevant studies, followed by a thorough full-text assessment of the selected articles. Both screening stages were performed independently by two reviewers, with a third reviewer consulted to resolve any disagreements. To maintain methodological rigor and transparency, the process was conducted in line with the PRISMA 2020 guidelines.
A structured literature search was conducted independently by two reviewers using PubMed, Cochrane CENTRAL, Scopus, PEDro, and Web of Science. The search was performed between 1 September 2024 and 23 January 2025, with disagreements resolved by a third reviewer.
2.6. Data Extraction and Data Synthesis
Data extraction was systematically performed to gather essential information, including study design, participant characteristics, intervention specifics, reported outcomes, and key findings. A standardized extraction form was employed to ensure consistency across studies, facilitating uniform data collection. Outcomes were organized to enable comparative analysis, with qualitative evaluation used to identify recurring patterns and gaps within the literature. Additionally, quantitative data were synthesized to highlight notable trends and significant results. This structured approach allowed for a comprehensive and methodologically rigorous synthesis aligned with the study objectives.
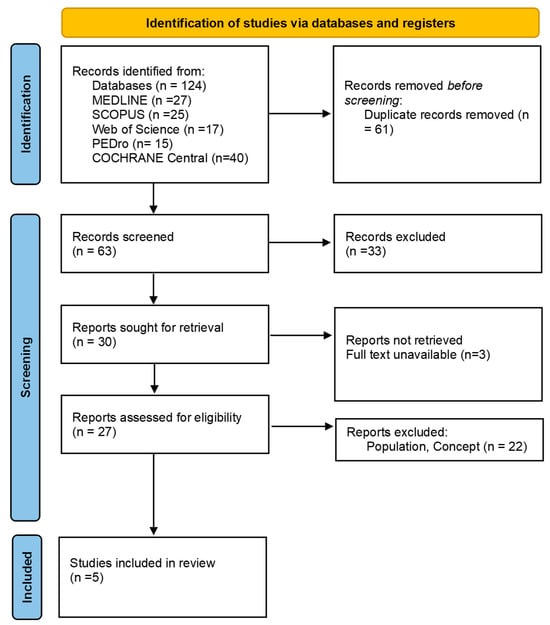
3. Results
As presented in
Figure 1 (PRISMA 2020 flow diagram), from the records identified by the initial literature searches, 119 studies were excluded, and 5 articles met the inclusion criteria (
Table 1).
3.1. Pain Reduction
Pain relief was one of the most consistently reported outcomes across the studies, with varying degrees of effectiveness depending on the intervention type. The study by Aoyama et al. (2019) [
47] demonstrated that patients who engaged in trunk stabilization exercises alongside pelvic strengthening reported significantly greater pain reductions compared to those who performed pelvic strengthening alone. This effect was particularly evident at the eight-week follow-up, suggesting that core stability plays a crucial role in reducing discomfort associated with FAIS. Similarly, Kemp et al. (2021) [
19] found that a progressive strengthening and functional training program led to greater pain relief than a control group that followed a standardized stretching and physical activity program, emphasizing the importance of targeted resistance training and neuromuscular re-education in pain management.
Mansell et al. (2018) [
5] compared pain relief outcomes between physiotherapy and arthroscopic surgery and found no significant difference between the two groups at the two-year follow-up. Both groups experienced sustained reductions in pain, reinforcing the idea that conservative treatment can be equally effective as surgery in long-term pain management. However, Martin et al. (2021) [
29] reported that, at the twelve-month follow-up, patients who underwent arthroscopic surgery had greater reductions in pain compared to those who received physiotherapy alone. Similarly, Palmer et al. (2019) [
48] observed that, while both surgical and physiotherapy groups experienced pain relief, the surgical group demonstrated greater improvements, particularly in activities that involved hip flexion.
These findings suggest that conservative rehabilitation, particularly when incorporating core stabilization and progressive strengthening, is effective in managing pain. While surgery may provide superior short-term pain relief, long-term differences between surgical and non-surgical approaches are minimal.
3.2. Functional Improvement
Functional recovery was assessed through measures of movement efficiency, daily activity performance, and return to sports. Aoyama et al. (2019) [
47] found that the group incorporating trunk stabilization exercises experienced superior functional gains compared to those who focused solely on pelvic strengthening. This suggests that interventions targeting core stability contribute to more effective rehabilitation outcomes. Kemp et al. (2021) [
19] observed that patients in the progressive strengthening and functional training group demonstrated significant improvements in their ability to perform daily activities and sports-related movements, as measured by the International Hip Outcome Tool (iHOT-33). In contrast, the control group, which engaged in stretching and general physical activity, reported lower functional scores.
Mansell et al. (2018) [
5] found that, at the two-year follow-up, there were no significant differences in functional improvement between the surgical and physiotherapy groups, further supporting the idea that conservative rehabilitation is a viable alternative to surgery. However, Martin et al. (2021) [
29] observed that, after twelve months, the surgical group demonstrated greater improvements in their ability to return to sports and perform activities of daily living (ADLs) compared to those who received only physiotherapy. Palmer et al. (2019) [
48] found that, while surgery resulted in superior functional improvements, particularly in hip flexion-related activities, no major differences were found in other movement-related functions when compared to structured rehabilitation.
These results indicate that structured rehabilitation programs, particularly those incorporating progressive strengthening and functional training, can significantly improve functional performance. While surgery may accelerate functional recovery in the short term, long-term differences between the two approaches are not substantial.
3.3. Range-of-Motion (ROM) Improvement
Hip mobility and range-of-motion (ROM) restoration were important outcomes assessed across studies. Aoyama et al. (2019) [
47] reported that participants in the trunk stabilization group demonstrated greater improvements in hip flexion and internal rotation ROM compared to those who performed pelvic strengthening alone. Kemp et al. (2021) [
19] primarily focused on movement efficiency rather than specific ROM outcomes, though general improvements in mobility were observed in the strengthening group.
Mansell et al. (2016) [
5] found no significant differences in ROM between the surgical and physiotherapy groups at the two-year follow-up, indicating that both interventions led to similar long-term mobility improvements. Martin et al. (2021) [
29] observed that the surgical group showed significantly better ROM outcomes in hip flexion and abduction, though differences in other movement directions were not statistically significant. Similarly, Palmer et al. (2019) [
48] found that, while the surgical group exhibited greater gains in hip flexion ROM, no major differences were noted in other directions when compared to physiotherapy.
Overall, these findings suggest that both conservative and surgical treatments improve ROM, though surgery appears to offer greater short-term improvements in hip flexion. Exercise-based rehabilitation, particularly core stabilization and targeted mobility training, remains an effective approach for enhancing overall movement efficiency.
3.4. Muscle Strength Gains
Muscle strength was a critical outcome assessed across studies, particularly in relation to hip and core stabilization. Aoyama et al. (2019) [
47] found that participants who engaged in trunk stabilization exercises exhibited significantly greater improvements in hip flexor and abductor strength compared to those who focused only on pelvic strengthening. Kemp et al. (2021) [
19] reported that participants in the progressive strengthening program demonstrated greater gains in hip and core muscle strength, which directly correlated with improved functional performance.
Mansell et al. (2018) [
5] found that both surgical and physiotherapy groups experienced muscle strength improvements, though no significant differences were observed between the two approaches at the two-year follow-up. Martin et al. (2021) [
29] reported that patients who underwent surgery showed superior strength gains, particularly in hip extensors and stabilizers, compared to those in the physiotherapy group at twelve months. Palmer et al. (2019) [
48] found that the surgical group had greater improvements in hip flexion and abduction strength, though core stability gains were more pronounced in the physiotherapy group.
These findings suggest that, while surgery may lead to greater improvements in hip-specific strength, physiotherapy-based interventions focusing on core stability and functional strengthening are highly effective in increasing muscle strength, which plays a key role in improving postural stability and movement efficiency.
3.5. Quality-of-Life Improvement
Quality of life (QoL) was assessed using patient-reported outcome measures such as the International Hip Outcome Tool (iHOT-33) and the modified Harris Hip Score (mHHS). Aoyama et al. (2019) [
47] found that participants in the trunk stabilization group reported higher QoL scores, which were associated with better pain relief and functional improvements. Kemp et al. (2021) [
19] reported that patients in the strengthening and functional training group demonstrated significantly better QoL outcomes, as measured by iHOT-33, compared to those in the control group.
Mansell et al. (2018) [
5] found no significant differences in QoL between the surgical and physiotherapy groups at the two-year follow-up, suggesting that both interventions lead to comparable long-term patient satisfaction. Martin et al. (2021 [
29]) observed that, at twelve months, patients who underwent surgery reported higher QoL scores than those in the physiotherapy group. Similarly, Palmer et al. (2019) [
48] found that, while the surgical group initially demonstrated greater QoL improvements, the differences between the two treatment groups diminished over time, indicating that structured rehabilitation can achieve comparable long-term outcomes.
These findings indicate that both surgical and conservative treatments improve QoL, with rehabilitation-based interventions demonstrating sustained benefits. While surgery may provide a faster initial improvement, structured rehabilitation remains a viable alternative for achieving long-term patient satisfaction.
4. Discussion
The findings of this scoping review provide valuable insights into the comparative effectiveness of rehabilitation strategies, including physiotherapy-based interventions, and surgical treatments for Femoroacetabular Impingement Syndrome (FAIS). The studies reviewed highlight the benefits of conservative rehabilitation approaches for FAIS, particularly in pain reduction, functional improvement, range-of-motion (ROM) restoration, muscle strength gains, and quality-of-life enhancement. While surgical treatment is available, this review focuses on non-surgical strategies and their clinical implications.
Pain reduction was a key outcome assessed in this review, alongside functional improvement and quality of life. Evidence suggests that both surgical and conservative interventions contribute to significant symptom relief, but rehabilitation strategies may also enhance function and long-term mobility. The observed improvements in pain and function following conservative rehabilitation may be attributed to the modulation of mechanical stress at the femoroacetabular interface. FAIS is characterized by abnormal contact between the femoral head and acetabulum due to cam or pincer deformities, leading to altered joint mechanics, chondral damage, and progressive loss of function. The resulting mechanical stress triggers synovial inflammation and contributes to pain, movement restrictions, and functional impairment. Strengthening exercises targeting the hip stabilizers, particularly the gluteal and deep core muscles, may reduce excessive joint loading and improve movement efficiency. Additionally, neuromuscular training and motor control exercises could enhance proprioception and dynamic stability, further mitigating symptoms associated with FAIS [
23,
49,
50].
The studies by Aoyama et al. and Kemp et al. [
19] demonstrated that structured physiotherapy-based interventions, particularly those incorporating core stabilization, strengthening, and functional training, effectively reduce pain over time. The role of neuromuscular control appears particularly relevant in the conservative management of FAIS, as targeting hip and trunk stability may alleviate mechanical stress on the affected joint structures. Conversely, studies such as those by Martin et al. [
29] and Palmer et al. [
40] indicated that surgery offers more immediate pain relief, particularly in the short term, with patients reporting greater reductions in discomfort at the twelve-month follow-up compared to those receiving only physiotherapy. However, long-term follow-ups, such as those by Mansell et al. [
5], suggest that the differences between surgical and non-surgical pain relief outcomes become less pronounced over time. This raises the question of whether surgical intervention is necessary for all FAIS cases or if well-structured rehabilitation programs could be sufficient for many patients.
Functional improvement represents another key measure in determining treatment effectiveness. Studies that incorporated progressive resistance training, physiotherapy-based rehabilitation, and motor control exercises, such as those by Kemp et al. [
19] and Aoyama et al. [
39], showed that conservative interventions effectively enhance mobility and movement efficiency. Patients undergoing structured rehabilitation reported significant improvements in their ability to perform daily activities and return to sport, which supports the growing recognition of physiotherapy as a primary intervention for FAIS. The inclusion of dynamic neuromuscular training and postural retraining further strengthens the argument for non-surgical management. However, given the heterogeneity in rehabilitation protocols across studies, it is important to interpret the results with caution, as different interventions may lead to varying outcomes based on individual patient characteristics and baseline functional status.
On the other hand, studies such as Martin et al. [
25] and Palmer et al. [
48] demonstrated that patients who underwent arthroscopic surgery achieved superior functional gains, particularly in hip flexion-related movements, within the first year of treatment. However, the long-term comparison provided by Mansell et al. [
5] indicated that these advantages diminished over time, suggesting that surgical intervention may primarily serve to accelerate early-stage functional recovery rather than provide additional long-term benefits.
Range-of-motion (ROM) restoration was another important factor in evaluating the efficacy of different treatment approaches. The studies reviewed indicate that surgery is particularly effective in improving hip flexion and abduction, as evidenced by Martin et al. [
25] and Palmer et al. [
48]. However, Aoyama et al. [
47] demonstrated that conservative approaches incorporating trunk stabilization exercises also resulted in meaningful gains in hip ROM, particularly in flexion and internal rotation. The absence of significant long-term differences in ROM between surgical and non-surgical groups in the study by Mansell et al. [
5] suggests that, while surgery may facilitate faster improvements, rehabilitation-focused interventions can achieve similar outcomes with sufficient time. This finding supports the notion that non-operative management, when tailored appropriately to individual patients, may serve as an effective first-line approach for restoring mobility in FAIS.
Muscle strength is another crucial aspect of rehabilitation, particularly given the role of hip and core musculature in stabilizing the joint and mitigating excessive stress on the femoroacetabular interface. Studies by Aoyama et al. [
47] and Kemp et al. [
19] demonstrated that progressive strengthening interventions lead to substantial improvements in hip flexor and abductor strength, which directly correlated with enhanced functional outcomes. In contrast, Martin et al. [
29] and Palmer et al. [
48] reported that surgical patients exhibited superior strength gains, particularly in hip extensors and stabilizers, at twelve months. While this suggests that surgery may allow for more rapid muscle adaptation, the finding that core stability improvements were more pronounced in the physiotherapy group in the study by Palmer et al. [
48] reinforces the importance of targeted rehabilitation strategies. Strength gains associated with physiotherapy are likely due to increased neuromuscular activation and motor control improvements rather than solely muscle hypertrophy, emphasizing the need for well-designed exercise programs tailored to FAIS patients.
Quality-of-life outcomes further reinforce the potential of conservative rehabilitation as an effective treatment option. While studies such as those by Martin et al. [
29] and Palmer et al. [
48] reported superior quality-of-life scores for surgical patients at the twelve-month mark, long-term follow-ups demonstrated a narrowing of differences between surgical and non-surgical groups. Aoyama et al. [
47] and Kemp et al. [
19] showed that structured rehabilitation interventions led to significant and sustained improvements in patient-reported quality of life, particularly when exercise programs were designed to address functional limitations and pain management. The absence of long-term differences in quality-of-life outcomes in the study by Mansell et al. [
5] suggests that physiotherapy, when appropriately applied, can provide comparable long-term benefits to surgery. This finding is particularly relevant in the context of healthcare resource allocation, as it highlights the potential for high-quality rehabilitation programs to serve as a cost-effective alternative to surgical intervention in select patient populations.
Taken together, the findings of this review support the growing body of evidence suggesting that conservative rehabilitation should be considered a primary intervention for FAIS, particularly in cases where surgery is not immediately indicated [
48]. While arthroscopic procedures may facilitate faster improvements in pain, function, and ROM in the short term, long-term differences between surgical and non-surgical outcomes are less substantial. Given the risks associated with surgical intervention, including post-operative complications and prolonged recovery periods, structured physiotherapy programs that incorporate core stabilization, progressive strengthening, and neuromuscular training offer a viable alternative for many patients. Future research should focus on defining standardized conservative treatment protocols and optimizing rehabilitation strategies to ensure the best possible outcomes for FAIS patients.
5. Limitations
Several limitations should be considered when interpreting the findings of this review. One key limitation is the heterogeneity among studies in terms of intervention protocols, outcome measures, and follow-up durations. The included studies varied significantly in their approach to rehabilitation, with some focusing on strengthening and motor control exercises, while others incorporated manual therapy or neuromuscular training. This variability makes direct comparisons challenging and limits the ability to establish standardized rehabilitation guidelines for FAIS. Additionally, follow-up periods ranged from a few months to two years, making it difficult to determine the long-term sustainability of the observed improvements, particularly in pain relief and functional recovery.
Another limitation is the inconsistency in diagnostic criteria across studies. While some trials used the imaging-based confirmation of FAIS, others relied on clinical examination alone, potentially leading to variability in patient selection. This heterogeneity raises concerns about the generalizability of findings, as patients with different structural presentations or symptom severity may respond differently to treatment. Furthermore, most studies included relatively small sample sizes, which may have limited their statistical power to detect subtle but clinically relevant differences between treatment approaches. The reliance on patient-reported outcomes also introduces potential bias, as the subjective assessments of pain and function may be influenced by individual expectations and placebo effects.
Lastly, the lack of standardized rehabilitation protocols across studies limits the ability to determine the most effective combination of conservative treatments. While some studies demonstrated strong outcomes with exercise therapy alone, others included multimodal interventions, making it difficult to isolate the effects of specific rehabilitation components. Future research should aim to develop more standardized physiotherapy protocols and identify patient subgroups that may benefit most from conservative management.
6. Clinical Practice Implications
The findings of this review have important implications for clinical practice, particularly in the management of FAIS. Given the comparable long-term outcomes between conservative rehabilitation and surgery, physiotherapy should be considered a first-line treatment for most patients before opting for surgical intervention. Structured rehabilitation programs incorporating core stability, progressive muscle strengthening, and neuromuscular training have been shown to improve pain, function, and quality of life, making them essential components of FAIS management. Clinicians should prioritize individualized exercise programs tailored to the patient’s specific movement deficits and functional limitations, as targeted interventions appear to yield better outcomes than generic stretching or passive treatments.
For patients with severe pain, functional impairments, or failure to respond to conservative treatment, surgery may still be a viable option. However, given the associated risks and recovery time, clinicians should ensure that patients have undergone an adequate trial of physiotherapy before considering arthroscopic intervention. The evidence supporting surgery as a superior option is strongest in the short term, particularly for pain relief and ROM improvements, but long-term differences compared to rehabilitation alone are less pronounced. This highlights the importance of shared decision making between patients and healthcare providers, ensuring that treatment choices align with patient preferences, activity levels, and clinical presentation.
Additionally, this review underscores the need for standardized rehabilitation protocols to optimize conservative management. Future guidelines should emphasize the integration of core stabilization, movement retraining, and functional strengthening into rehabilitation programs, as these elements have demonstrated positive effects on pain reduction and functional recovery. By refining conservative treatment strategies and identifying key predictors of successful non-surgical outcomes, clinicians can better tailor interventions to meet the needs of FAIS patients, potentially reducing the need for surgical intervention in many cases.