1. Introduction
Cervical lordosis is the anterior convexity of the cervical spine, which extends from the foramen magnum to the first thoracic vertebra. Normal cervical curvature is lordotic, and proper cervical curvature is important for good posture and function of the head and neck area [
1,
2].
Loss of normal cervical curvature is relatively common. Previous studies have reported that only one-third of the adult population shows lordotic cervical curvature, while the rest show straight, kyphotic (curved in the opposite direction of lordosis), or sigmoid (which has both lordotic and kyphotic curves) cervical curvature [
3,
4,
5]. Loss of the normal cervical curvature can cause neurological symptoms, neck and shoulder pain, headaches, and other disorders, thus causing functional disability [
1,
6,
7,
8,
9]. Although there are many studies on the biomechanical changes that alter cervical curvature, the exact pathophysiology has not been established. It has been reported that cervical curvature can be affected by numerous factors, such as age, sex, trauma, congenital defects, cervical muscle weakness, tumors, infection, and psychosocial factors [
2,
4,
10,
11,
12]. Recently, interest has been focused on the relationship between cervical curvature and posture because forward head posture is common with the use of smartphones [
13,
14]. Forward head posture is a habitual neck posture defined by forward translation of the cervical spine and is thought to be related to cervical curvature malalignment. As the head tilt is more forward in relation to the cervical spine, the axial load moves anteriorly. Consequently, increased compressive force can trigger a progressive degenerative process and potentially result in poor alignment of the cervical curvature [
15].
Few studies have investigated the relationship between craniofacial characteristics and cervical posture [
16,
17]. Hellsing et al. [
16] reported that subjects between ages 8 and 15 years with dolichocephalic faces had a forwardly inclined cervical column. Similarly, Solow and Tallgren [
17] investigated adult males between the ages of 18 and 30 and reported that forward head posture was frequently associated with a large anterior facial height, maxillary and mandibular retrognathism, and large mandibular plane inclination. However, to our knowledge, there have been no studies on the relationship between vertical facial patterns and craniocervical posture in adult females.
Cervical curvature can be associated with craniocervical posture and vertical facial patterns. A few studies have investigated cervical curvature variations according to vertical facial patterns, and the results are controversial [
8,
16,
17,
18]. No studies have compared the distribution of cervical curvature type according to different vertical facial patterns. Our study is the first to establish a relationship between cervical curvature and vertical facial patterns. The purposes of this study were to (1) compare the craniocervical posture of adult females with different vertical facial patterns, (2) compare the distribution of cervical curvature variations with different vertical facial patterns, and (3) determine any correlation between the vertical facial pattern, craniocervical posture, and cervical curvature measurements.
4. Discussion
The relationship between the sagittal facial patterns and the type of cervical curvature remains controversial [
16,
17,
31]. To exclude the effects of the anteroposterior skeletal discrepancy on the type of cervical curvature, we only investigated patients with a skeletal Class I relationship.
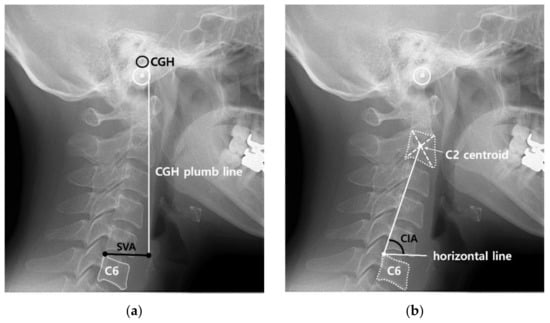
This study used two measurements of craniocervical posture (SVA and CIA) and three methods of cervical curvature (Ohara, Cobb, and Harrison posterior tangent methods). Introduced in 1889, SVA is the most commonly used method to measure the anteroposterior head position. However, it has the limitation of being affected by individual size differences [
21]. Therefore, the CIA method, which measures the degree of head tilt, was used. However, the CIA considers only the position of the cervical vertebrae and does not use any reference to the head. Both methods were employed to evaluate craniocervical posture for a more accurate analysis. The Cobb method is the most widely used method for cervical curvature measurement because of its ease of use and good intra- and interrater reliability. The Harrison posterior tangent method is the most accurate method for measuring cervical curvature [
1,
28]. However, as angular methods primarily assess overall curvature, they cannot effectively distinguish segmental reversed curvatures (sigmoid) from lordotic or straight alignments; therefore, the Ohara method, which can distinguish regional kyphotic curvatures, was also utilized [
32].
Based on SVA and CIA values, the hyperdivergent group was distinguished from the other groups. The hyperdivergent group showed a more anterior position of the head and increased anterior inclination of the cervical spine than the hypodivergent group. Our findings are similar to previous studies that reported a correlation between large vertical craniofacial dimensions and extended head posture [
17,
33,
34,
35]. This mechanism can be explained by ‘neuromuscular feedback’ and is termed the ‘soft-tissue stretching hypothesis’. This hypothesis suggests that the soft tissue layer is passively stretched when the head is extended relative to the cervical vertebral column. This would increase forces on the skeletal structures and could redirect the mandibular growth more caudally [
31]. Consequently, subjects with a hyperdivergent facial pattern or a retrognathic profile are likelier to exhibit a forward craniocervical posture.
The three groups had no significant differences in the Cobb angle and Harrison posterior tangent angle. As these angles serve as criteria for classifying cervical types, comparing these angles between the three groups when all cervical curvature types are intermixed seems to have no clinical significance. For this reason, it would be more meaningful to ascertain the distribution of cervical curvature types for each vertical facial pattern and compare the differences in these distributions.
Cervical curvature was classified into four categories within each group. It is well accepted that the physiological cervical curvature is lordotic in a natural head posture. However, our results showed that only 19.6% of the samples had lordotic cervical curvature. A straight cervical curvature was the most common (48.9%), followed by kyphotic (25.0%), lordotic (19.6%), and sigmoid (6.0%) curvatures. In previous studies, lordotic cervical curvature was not dominant. Beltsios et al. [
4] conducted a study on 100 healthy adults and reported that approximately one-third of the population had a lordotic cervical spine, one-third had a straight spine, and the remaining third had either kyphotic or sigmoid curvatures. Yu et al. [
3] reported that 28% of young asymptomatic Chinese adults have lordotic cervical spines, whereas 45% have straight spines. Nonetheless, compared to previous findings [
3,
4], our results indicate a lower proportion of lordotic cervical curvature.
This is the first study to describe the prevalence of each type of cervical curvature in different vertical facial patterns. In the hypodivergent and hyperdivergent groups, the straight curve was most prominent, whereas in the normovergent group, the lordotic curve was predominant. Fisher’s exact test indicated an association between the vertical facial pattern and the type of cervical curve. The normovergent group had a higher frequency of lordotic curves and fewer straight curves, the hypodivergent group had a predominance of straight curves, and the hyperdivergent group had fewer lordotic curves. Compared with previous studies [
3,
4,
36], the distribution of cervical curvature types in the normovergent group was similar, but the hypodivergent and hyperdivergent groups showed a higher proportion of non-lordotic cervical curvatures. In this study, although there were no significant differences in the mean values of cervical curvature measurements, the distribution of cervical curvature types showed a significant difference between the three groups. This may be linked to the observation that the hypodivergent group had the highest proportion of straight curves and the lowest proportion of kyphotic curves, whereas the normovergent group had an even distribution for each curvature type. As expected, there was a greater prevalence of non-lordotic cervical curvature in the hyperdivergent group, which tended to show a forward head posture. However, the hypodivergent group showed a greater prevalence of straight curvature. Fineman et al. [
37] reported that subjects who changed from a neutral position to a military posture (backward craniocervical posture) often experienced the loss of cervical lordosis, leading to a straight cervical alignment. Variations in muscle tension around the shoulder and neck areas may contribute to this phenomenon [
38]. In addition, craniofacial development is closely linked to stomatognathic functions, such as mastication, swallowing, and respiration, all of which influence craniocervical posture [
39,
40]. Further research is needed to investigate their biomechanical impact on cervical alignment, with biomechanical analysis and longitudinal studies providing further validation of these relationships.
In this study, we investigated the correlations among NSL/ML, craniocervical posture, and cervical curvature. The Pearson correlation suggests that the NSL/ML showed a moderate correlation with craniocervical posture, implying that head and cervical postures may vary according to the vertical facial pattern, aligning with the aforementioned soft-tissue stretching hypotheses. Thus, an increase in the mandibular plane angle was associated with a more anterior positioning of the head and neck. Our results showed a weak negative correlation between NSL/ML and cervical curvature measurements. This suggests that an increase in the mandibular plane angle corresponds to a decrease in cervical curvature; however, when examining the distribution of cervical curvature types, no difference was observed between the hyperdivergent and hypodivergent groups. Tecco et al. [
8] found no significant differences in cervical curvature relative to vertical facial patterns. Their study was limited in not including kyphotic cervical curvature since kyphosis is not considered a physiological posture of the spine. Solow and Tallgren [
17] observed a very weak negative correlation between the mandibular plane angle and cervical lordosis angle (the angle between odontoid process tangent and a line through the inferoposterior points of C2 and C4, CLA), noting reduced CLA in association with large vertical facial dimensions and increased CLA with a shorter vertical dimension. However, these studies were conducted with adult men; therefore, the results cannot be directly compared with those in our study. This indicates that the cervical curvature type cannot be explained solely by the magnitude of the mandibular plane angle. Examination of the relationship between craniocervical posture and cervical curvature measurements revealed that the Cobb angle had a weak correlation with craniocervical posture, whereas the Harrison posterior tangent angle showed no correlation. There are two possible explanations for this minimal correlation. First, a backward craniocervical posture may affect cervical curvature. Typically, a more lordotic curvature is expected with a more backward head position; however, this study found a prevalence of straight curvatures associated with such a posture. Second, cervical curvature may be influenced by multiple factors, with craniocervical posture being one of many potential influences. Previous studies suggest that factors such as muscle tension, lifestyle patterns, repetitive trauma, and congenital and developmental conditions may play a role [
9,
41,
42,
43], rather than craniofacial structure alone. This may explain the weak correlation observed in the present study. Additionally, the influence of environmental and social factors remains unclear, requiring further research on physical, psychosocial, and personal risk factors to better understand their impact on cervical alignment.
The mechanism underlying loss of cervical lordosis remains unclear. A recent hypothesis is that weakness of the neck extensor muscles is a risk factor for the development of cervical kyphosis [
44]. A previous study has reported on the association between forward head posture and neck muscle imbalance [
45]. Therefore, it is reasonable to assume that neck muscle imbalance according to different cervical postures may affect cervical spine curvature. To date, no trial has investigated the differences in neck extensor and flexor muscles according to vertical facial patterns. Only partial neck muscles were investigated, and they reported significant differences in the electromyographic activity of the sternocleidomastoid and trapezius when the vertical dimension varied [
46]. Therefore, cervical muscle status according to vertical craniofacial factors should be considered in future studies.
Many dental clinicians are not familiar with methods for assessing cervical spine alignment. This study found that the simple Cobb method showed a strong correlation with the highly accurate Harrison method, making it a clinically accessible diagnostic tool. This correlation is likely due to both methods relying on angular measurements, which primarily evaluate overall cervical curvature. However, discrepancies between methods arise because angular measurements alone cannot differentiate segmental reversed curvatures, whereas the Ohara method, using linear assessments, is more sensitive to detecting regional kyphotic changes. Therefore, incorporating linear assessments alongside angular methods may enhance diagnostic accuracy in clinical practice.
This study had certain limitations. First, this study is limited to adult females aged 18–35 years, and further research is needed to explore cervical curvature in males and other age groups to improve generalizability. Second, the seventh cervical vertebrae were excluded from the analysis. In practice, seeing the lower cervical spine on routine lateral cephalometric radiographs is difficult. While three methods were used to address this limitation, the exclusion of C7 may impact the completeness of cervical curvature evaluation. To improve the evaluation of cervical curvature, future studies should consider adjusting imaging techniques to include the lower cervical spine. Third, various factors may influence cervical spine alignment, necessitating further investigation into biomechanical elements, such as daily life habits or job. Despite these limitations, this study is pioneering in illustrating the variance in cervical curvature types across vertical facial patterns. It has also been established that craniofacial features contribute to craniocervical posture and cervical curvature, although the exact nature of the cause-and-effect relationship remains unclear. Cervical posture is associated with facial soft-tissue aesthetics, while cervical spine curvature affects health-related quality of life [
25]. Consequently, this study suggests that clinicians should meticulously evaluate craniocervical posture and cervical spine curvature using routine lateral cephalometric radiographs prior to orthodontic treatment.