1. Introduction
The World Health Organization (WHO) estimates that around 16% of the population of any country has some disability (around 1.3 billion people; 1 in 6 people). It is estimated that around 5% are people with mental disabilities, 2% with physical disabilities, 1.5% with hearing impairment, 0.5% with visual impairment, and 1% with multiple disabilities [
1]. People with special needs encounter challenges such as physical barriers, social inclusion, educational adaptation, daily activities, and personal hygiene [
2]. Encouraging healthy living and autonomy must be developed, using adaptations and alternatives. Therefore, maintaining adequate oral hygiene can be difficult for these individuals [
2,
3].
Chronic diseases have a pronounced worldwide prevalence and are an evident public health concern. Moreover, it was proposed that diseases from the oral cavity and systemic diseases have a bidirectional association [
4,
5,
6,
7,
8]. While evidence of this bidirectional link is robust in diseases that limit oral self-care (either physical or cognitive incapacity), the association of oral diseases with other chronic noncommunicable diseases (NCDs) has increased, still without the proper consistency.
However, there is a need for programs that can develop methods of motivation and oral health literacy adapted for this part of the population so lacking in information and alternatives to adapt to their reality, establishing a routine of prevention, guidance, and knowledge about oral hygiene [
9]. The development of oral health education programs and strategies is of utmost importance for patients with special needs, aiming to reduce the rates of tooth decay and periodontal disease rates, which are generally prevalent [
2,
3,
9]. Adaptations and appropriate care can generate motivation for health and constitute autonomy for these patients. This encouragement of independence and self-care contributes to oral health and general health, which is the motivation and benefit of being healthy [
2,
3,
9,
10,
11]. Thus, aiming to promote increased knowledge, oral health education programs help reduce risk factors for oral diseases, promoting the control of dental biofilm and the consumption of a healthy diet [
10]. A significant barrier to preventing major oral diseases would be the lack of knowledge, inadequate eating habits, and poor oral hygiene, which are the main factors for the development of tooth decay and periodontal disease.
Oral health literacy strategies aim to increase knowledge and encourage behavior, self-care, and diet changes [
12]. However, acquiring knowledge does not mean an immediate improvement in practices and attitudes. The complement includes education and prevention for oral health to be applied periodically [
9,
10,
11,
12]. Studies reveal that many people with special needs have never had adequate guidance on brushing and hygiene techniques, which is a worrying fact, as these individuals generally need special help or adaptations to learn how to perform their hygiene and, for example, adequately use a brush or dental floss [
3,
9,
10,
11]. Faced with the new global scenario, with the pandemic and social isolation, the internet has become an environment with an essential role in building connections, as well as bringing people together and spreading knowledge for the population, especially for those with some special needs [
13]. When correctly used, it becomes a favorable way for educational and cultural activities [
10,
11], as the ease of access and sharing of information allows a large portion of the population to be reached without the need to travel to a specific location [
12,
13]. Thereby, important and safe information about oral and general health care can be disseminated through the virtual environment. On the other hand, the work can become more comprehensive and exhaustive, as new content is needed with a certain frequency and the audience becomes heterogeneous, given the scope and diversity of the internet environment [
13,
14].
Social and research networks provide an environment for searching for health information. Data show that 80% of searches and browsing activities on the internet are directed toward health-related knowledge. The YouTube platform is the most popular platform for patients to consult to find health-related information, including information on oral health. However, not all information contained on YouTube is true or accurate, which may have a negative impact on the population’s health [
15]. Much of the dental content is published on digital platforms (Google, Facebook, YouTube, and Instagram), which may influence positively and/or negatively the patient’s vision, with reliable and unreliable information being available, which can lead to misunderstanding by the population. For this reason, it is essential to review these contents and check their reliability [
16].
Also, the application of digital technologies, such as augmented reality, virtual reality, and mixed reality, has led to advances in oral health. These applications permit the development of specific oral health literacy strategies focused on the most vulnerable social risk groups [
17].
Oral diseases affect almost half the world’s population, causing a substantial economic burden. Oral health promotion is one of the most cost-effective methods to overcome this problem. Digital media can play a fundamental role in reducing this burden, providing a broader platform to reach the entire population, regardless of their characteristics, and even in areas where oral health services are lacking [
17,
18]. Although oral health literacy is widely debated and has many heterogeneous conceptualizations, people with special health needs have often been neglected [
18]. There are many different approaches to preventing oral disease, and the most effective method in terms of costs is health promotion and education [
19]. As access to digital media continues to expand, it will increasingly serve as a valuable health resource in environments lacking specialized health knowledge. They are an alternative platform that can help reach people with special health needs, promoting greater oral health literacy. Evidence reveals that interactive digital interventions increase knowledge about oral health and change behaviors, constituting one of the main approaches to promoting oral health literacy [
20].
Thus, within this context, this study aimed to systematically review the use of new technologies and digital innovations to improve health literacy in patients with special needs and in vulnerable communities.
4. Discussion
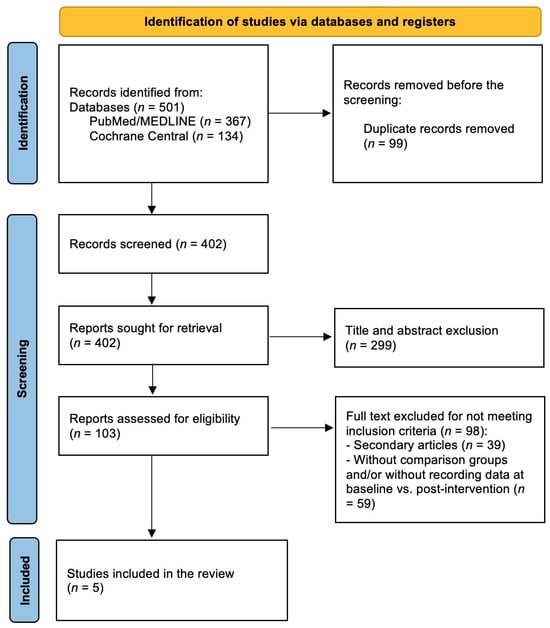
The main objective of this study was to identify the improvement of oral health literacy in patients with special needs and vulnerable communities using new technologies and innovations. Five articles were considered in the systematic review, presenting con-sensual views on the effectiveness of new technologies and innovations in promoting oral health literacy in patients with special health needs. As the focus of health care has shifted from treating disease to preserving health (preventive approach), health promotion has emerged as a social issue that affects individuals in general and health care professionals, whatever their field of practice.
In recent decades, there has been an increase in the use of the internet and digital devices, which has led to their integration into oral health care [
18]. Veiga et al. [
30] showed that using technological resources in health is essential. They improve communication and the reception of new information, permit more accessible communication, and, for leisure, improve feelings of loneliness and/or social isolation. Thus, eHealth was defined as health services and information transmitted through electronic and digital means. The eHealth conceptual model adequately integrates technology and health care, the benefits of which include increasing the effectiveness and accessibility of medical and dental services, for example, the implementation of various mobile health applications. With the help of the internet, people who face difficulties in accessing medical services can obtain health information and receive assistance to manage their oral health [
31,
32,
33]. This makes oral health care more accessible, especially for people living in remote areas or with mobility problems.
Additionally, eHealth technologies help reduce wait times, increase patient engagement in managing their oral health, and improve overall health outcomes [
2]. Currently, the internet is considered an essential source of health information. People who have difficulty obtaining medical and dental care can access health information online and receive assistance in managing their health condition. However, obtaining health-related information on the internet requires specific skills and health literacy, such as reading, understanding, and evaluating the information found, particularly on the part of people with special health needs [
2,
3,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
26,
27,
28,
29,
30]. Thus, the concept of eHealth Literacy emerged, defined as the ability to search, find, understand, and evaluate health information from electronic sources and apply the knowledge acquired to address or solve a health problem [
33].
The studies included in the present systematic review agreed that, in the field of oral health, the concept of health literacy has gained significant importance and has been integrated into oral health literacy, encompassing various tools and resources. Research has shown that individual and systemic factors influence oral health literacy. Personal factors such as education level, socioeconomic and cultural conditions, proficiency, and health literacy can affect a person’s ability to understand and use oral health information, whereas systemic factors include the complexity of access to health care and health systems. According to the values obtained after interventions using new technologies and innovations, all studies showed a significant increase in patients’ oral health literacy with special health needs. In the study ID 5 by Sharifard et al. [
29], the effectiveness of the ATP (audio-tactile performance) program for children/adolescents with visual impairments was demonstrated. Audio: verbal oral health education was offered to the target population on the importance of preventing oral diseases such as tooth decay and gum health. This program contained essential instructions for daily oral hygiene, with a verbal demonstration of techniques. The Art package consisted of an electronic game for oral health education based on music that complemented the ATP. Likewise, guidance/teaching to mothers via telephone completed the other interventions.
The study ID 1 by Pai Khot et al. [
25] included patients aged between 7 and 18 years old with ASD. The PAIR communication system, inspired by the Picture Exchange Communication System (PECS), was a modified version of the same that is based on descriptive data. It was a new pictorial system based on behavior, created to develop communication skills and educate children with special health needs in terms of oral hygiene practices, serving as a link with everyday practices. The PAIR intervention is based on the concepts of applied behavioral analysis and uses differentiated teaching and different teaching, reinforcement, and chaining strategies. Furthermore, this system uses pictorial differentiation of oral hygiene aids and structured illustrations, demonstrating oral hygiene tasks in different patterns with increased oral health literacy. This new digital technique contained illustrations in a sequence of actions necessary to maintain oral hygiene. The steps included were the following: step 1 was the illustration and identification of images by children/adolescents; step 2 was the illustrated object given to the children/adolescents to choose the correct image; step 3 was that children/adolescents identify the correct and incorrect illustrations presented; and step 4 was that children/adolescents produced a sentence following the sequence of images.
In the study ID 2 by Álvareza et al. [
26], the intervention was based on exercises with a Nintendo
® Wii™ TV and a Wii balance board in an experimental group. In contrast, the control group continued with their normal daily activities. The games applied on the Wii balance board challenge the stability of children with trisomy 21 by balancing their body weight, as requested by the game, causing a sensory and motor stimulus, which led the experimental group, after the intervention, to improve their postural control, resulting in greater ease in improving your oral hygiene. The data provided in this study demonstrated that when using an intervention based on the Wii balance board with appropriate adaptations to the characteristics of each child, children with trisomy 21 increased their knowledge about oral health and adopted behaviors that are more conducive to good oral health. One study by Genaro et al. [
34] found seeding results using virtual reality, where there was a significant increase in good oral hygiene practices. In the study ID 3 by Khalil et al. [
27], oral health literacy was a predictive factor for self-efficacy in oral health throughout each period of interventions, using smartphones with software applications for elderly people to read oral health messages. Likewise, Carli et al. [
28] found significant improvements between baseline and post-intervention values, that is, applying an oral health disease prevention program on personalized digital media, which significantly improved clinical parameters and patient behaviors.
As a limitation of this study, the low number of studies directly included that evaluated patients with special needs and technologies focused on oral health can be pointed out; moreover, it is possible to consider that the number of patients included in some of the articles was low and should be increased in future studies.