1. Introduction
Emotion regulation is a term used to describe “the processes by which individuals influence which emotions they have, when they have them, and how they experience and express them” [
1], (p. 275). Effective emotion regulation is associated with improved health and well-being [
2] and allows individuals to foster strong personal and professional relationships [
3]. Conversely, difficulties in emotion regulation are found to be a transdiagnostic risk factor for a wide range of psychopathologies [
4], including anxiety, depression, substance use, and eating disorders [
5]. Given its significance in mental health, accurately measuring difficulties in emotion regulation is crucial for both research and clinical practice.
The emotion regulation field is characterized by a variety of emotion regulation models and their corresponding measures. In a recent systematic review of emotion regulation models [
6], ten models were identified. The most prevalent model was the
process model of emotion regulation by Gross [
1,
7], with the Emotion Regulation Questionnaire [
8] and the Process Model of Emotion Regulation Questionnaire [
9] for measuring individual emotion regulation strategies (e.g., expressive suppression). The second most prevalent model was Gratz and Roemer’s model of difficulties in emotion regulation [
10]. It identifies four key components of emotion regulation: (1) recognizing and understanding one’s emotions, (2) accepting emotions, (3) managing behavior in alignment with goals while experiencing negative emotional states, and (4) using flexible, context-appropriate emotion regulation strategies to adjust emotional responses as needed to achieve personal goals and meet situational demands [
10]. Based on this model, the Difficulties in Emotion Regulation Scale (DERS) was developed [
10].
The DERS is one of the commonly used tools for assessing difficulties in emotion regulation (for review, see [
11,
12]). The original DERS-36 is a self-report questionnaire designed to assess six dimensions of difficulties in emotion regulation: (1) non-acceptance of emotional responses, (2) difficulties engaging in goal-directed behavior, (3) impulse control difficulties, (4) lack of emotional awareness, (5) limited access to emotion regulation strategies, and (6) lack of emotional clarity [
10,
13]. The DERS-36 is psychometrically reliable [
14], making it a cornerstone measure in both research and clinical contexts. Yet, with 36 items, the DERS-36 could be difficult to apply in certain situations or environments, such as large-scale epidemiological research or in a clinical treatment context [
14]. The previous evidence suggests that the DERS-36 performed similarly across gender (i.e., females vs. males) and racial groups, supporting meaningful comparisons between demographic groupings [
15,
16]. Females tended to have greater difficulties in emotion regulation than males; however, the effect size of gender differences was small (e.g., [
15,
17]).
In response, the DERS-8 was developed to assess difficulties in emotion regulation in both adolescents and adults [
18]. This brief, one-dimensional, eight-item self-report scale demonstrates strong psychometric properties [
18] while offering advantages in terms of its practical application. The reduced number of items makes the DERS-8 especially valuable in both clinical settings and long-term research supporting targeted interventions for older adults and providing precise emotional difficulties screening [
19]. Moreover, given their brevity, short scales are appropriate for studies where participants need to evaluate themselves and others multiple times [
20]. Furthermore, in some cases (e.g., online-based research, where respondents are unlikely to spend much time on the website), researchers may encounter constraints that force them to choose between using a very short tool or not measuring at all [
20]. Finally, the increasing pace of life, as well as specific research conditions, often forces researchers to work with progressively shorter tools, leading to an increasing need for such measures [
21].
Emotion regulation difficulties are suggested to be a transdiagnostic risk factor for a wide range of mental health issues [
4]. In Poland, the prevalence of such issues, including high levels of anxiety and depression symptoms as well as decreased levels of well-being, is high [
22,
23]. Therefore, a brief and effective psychometric tool for emotion regulation difficulties is of high relevance for research and clinical practice, chiefly a screening and prevention of mental health problems. As such, we deemed that the DERS-8 was a good candidate as a screening measure of emotion regulation difficulties in a Polish sample.
Given the above, the aim of the current study was to verify the psychometric properties of the first Polish version of the DERS-8 and to develop its current Polish norms. We hypothesized that
The Polish DERS-8 would be characterized by a one-factor structure, with a good fit in confirmatory factor analysis, and it would be invariant across different demographic categories as well as mental health outcomes levels;
The Polish DERS-8 would have good internal consistency reliability;
Higher difficulties in emotion regulation, measured with the Polish DERS-8, would be associated with higher levels of psychological distress (i.e., anxiety and depression symptoms) and lower levels of well-being, supporting convergent and divergent validity of the scale;
The Polish DERS-8 would show good discriminant validity, with its scores being statistically separable from psychological distress and well-being;
The Polish DERS-8 scores would be meaningful statistical predictors of anxiety and depression symptoms as well as psychological well-being while controlling for sociodemographic variables.
Making implications for the assessment and treatment of emotion regulation issues more accessible, we strove to present Polish adult norms for the DERS-8. To help facilitate the interpretation of the scale scores in research and practice, we presented a guide to their interpretation.
3. Results
3.1. Descriptive Analysis and Internal Consistency Reliability
Table 2 demonstrates descriptive statistics of the study variables across gender groups. All the study variables were reasonably normally distributed in the total sample (
n = 1329), with skewness values from 0.12 to 0.55 and kurtosis values from −1.11 to −0.34.
Internal consistency reliability of the DERS-8 was good, with McDonald’s Omega of 0.88 and Cronbach’s Alpha of 0.89. The other questionnaires also showed good reliability in this study, with omega and alpha coefficients of ≥0.79.
3.2. Factor Structure and Its Invariance
Descriptive statistics for the DERS-8 items are displayed in
Table 3.
The intended one-factor DERS-8 model had a good fit to the data (e.g., CFI = 0.986, RMSEA = 0.072, SRMR = 0.056, see
Table 4). All factor loadings were high (≥0.601, all
ps < 0.001, see
Table 3).
The one-factor DERS-8 model showed configural, metric, and scalar level invariance across all the tested demographic categories and psychological distress (PHQ-4) and well-being (WHO-5) levels, with the absolute difference of CFI being equal to 0.009 and less between the invariance levels (see
Table 4).
3.3. Convergent and Divergent Validity
As expected, DERS-8 scores were strongly positively associated with anxiety and depression symptoms and negatively with well-being (see
Table 5), supporting convergent and divergent validity.
3.4. Discriminant Validity
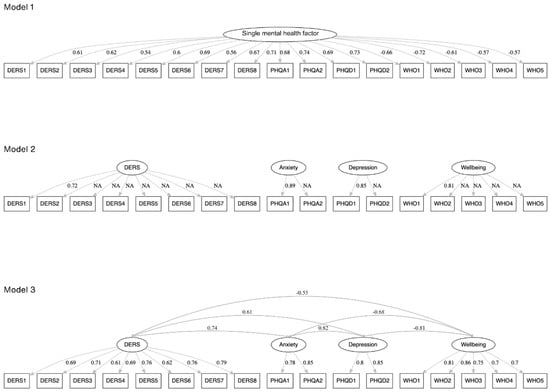
We conducted two series of confirmatory factor analyses to examine the discriminant validity of the DERS-8. We were interested in whether difficulties in emotion regulation were a statistically separable construct from anxiety and depression symptoms as well as well-being (see
Figure 1 with the tested models).
As expected, the single mental health factor model had a poor fit to the data. The four-factor model with uncorrelated (orthogonal) factors was not identified (see
Table 6); therefore, factor loadings could not be computed.
In contrast, the four-factor correlated model, with the separate DERS-8, PHQ-4 Anxiety, PHQ-4 Depression, and WHO-5 factors, had an excellent fit to the data. Therefore, our analysis showed that difficulties in emotion regulation were distinct from psychological distress and well-being. Additionally, the 95% CI for the estimated correlations between all the pairs of the examined constructs did not include 1.0, supporting evidence of discriminant validity for the constructs. Finally, AVE values were ≥0.57, and values of HTMT ratio of correlations were ≤0.81, further supporting good discriminant validity of the four constructs, as measured with the DERS-8, two PHQ-4 subscale scores, and WHO-5.
3.5. Predicting Mental Health Outcomes Based on DERS-8 Scores
The regression analysis demonstrated that DERS-8 scores, adjusting for demographic variables, were a strong positive predictor of anxiety and depression symptoms (beta = 0.60,
p < 0.001) and a strong negative predictor of well-being (beta = −0.47,
p < 0.001). Detailed results are displayed in
Table 7 and
Table 8.
3.5.1. Predicting Psychological Distress Based on DERS-8 Scores
In Step 2, among demographic variables, only relationship status was a statistically significant predictor of anxiety and depression symptoms, with being in relationships associated with less emotion regulation difficulties (see
Table 7). Beyond demographic variables, the DERS-8 scores explained 32.40% of the variance of anxiety and depression symptoms (Δ adjusted R
2 between Step 2 and Step 1).
3.5.2. Predicting Well-Being Based on DERS-8 Scores
In Step 2, among demographic variables, only relationship status was a statistically significant predictor of well-being, with being in relationships associated with higher levels of well-being (see
Table 8). Beyond demographic variables, the DERS-8 scores explained 19.44% of the variance of well-being (Δ adjusted R
2 between Step 2 and Step 1). Overall, our regression analyses showed that emotion regulation difficulties could statistically significantly predict negative and positive mental health outcomes.
3.6. Demographic Differences
We used three series of ANCOVAs (with age used as a covariate) to compare DERS-8 scores between (1) females and males, (2) people without university degrees and people with university degrees, and (3) singles and people in relationships. There were gender differences in emotion regulation difficulties, with females tending to have higher DERS-8 scores than males, F(1, 1288) = 28.24, p < 0.001, η2 = 0.02. People without university degrees tended to have higher DERS-8 scores than people with university degrees, F(1, 1326) = 4.79, p = 0.029, η2 = 0.003. Relationship status did not differentiate DERS-8 scores (p < 0.05). In all these three series of ANCOVAs, age was a statistically significant covariate. Pearson correlations demonstrated that age was negatively correlated with DERS-8 scores in females (r = −0.29, p < 0.001) and males (r = −0.28, p < 0.001), suggesting that younger people tended to have more emotion regulation difficulties.
3.7. Group Norms
We calculated group norms for the DERS-8 scores across the total sample and, due to age differences in emotion regulation difficulties, for two age groups (i.e., aged 18–29 and 30–73) separately (see
Supplementary Files).
4. Discussion
The aim of the study was to examine the psychometric properties of the Polish version of the DERS-8 and to present its norms. Overall, much like the original English version [
18], the Polish DERS-8 showed strong psychometric performance, including factorial validity, internal consistency reliability, and convergent, divergent, and discriminant validity.
4.1. Factor Structure and Measurement Invariance
As expected, the one-factor structure of the Polish DERS-8 was supported empirically in confirmatory factor analysis. The scale was also characterized by strict invariance across different demographic categories, including gender, age, education, and relationship status, supporting the possibility of comparing the mean DERS-8 scores between these demographic groups meaningfully. As a further contribution to the emotion regulation field, we also tested whether the DERS-8 structure was the same between people with different levels of mental health outcomes (i.e., between people with normal and high psychological distress levels and between people with normal and low well-being levels). In this case, our analysis also supported the strict invariance of the DERS-8, suggesting that regardless of different levels of mental health outcomes, difficulties in emotion regulation could be effectively measured with the Polish DERS-8. Our results are in line with the conclusions presented in the original DERS-8 paper [
18], where the scale showed strong replicability and clinical relevance in assessing emotion regulation difficulties between clinical and non-clinical samples. Taken together, the current empirical evidence suggests that the DERS-8 has demonstrated strong factorial validity across Penner et al.’s study [
18] and this Polish one. This evidence is promising; however, to the best authors’ knowledge, the Polish version of the scale seems to be the first non-English translated version of the tool. Therefore, more studies are required to investigate its factor structure across different cultural contexts.
4.2. Internal Consistency Reliability and Convergent, Divergent and Discriminant Validity
Consistent with the original DERS-8 validation study [
18], the internal consistency reliability of the total scale scores, as measured with McDonald’s Omega and Cronbach’s Alpha, was good. This indicates that the measurement of emotion regulation difficulties with the DERS-8 is robust, despite the tool’s brevity.
In terms of convergent and divergent validity, Penner et al. [
18] noted reasonable positive correlations between the DERS-8 scores and other negative mental health outcomes (e.g., borderline personality, internalizing and externalizing problems, etc.), somatic complaints, and neuroticism from the Big Five personality. In our study, we were interested in not only exploring whether emotion regulation difficulties were related to negative mental health outcomes but also whether these difficulties were related to a decline in well-being, serving as one of the positive mental health outcomes. In our Polish study with its bivariate correlational analysis, DERS-8 scores were strongly positively related to anxiety and depression symptoms and negatively related to well-being. The DERS-8 scores were more strongly associated with anxiety symptoms (
r = 0.62) than depression ones (
r = 0.51) and similarly strongly but negatively associated with well-being (
r = −0.48).
Despite these strong correlations between the constructs of interest (i.e., emotion regulation difficulties, psychological distress, and well-being), our discriminant validity analysis indicated that emotion regulation difficulties were statistically separable from psychological distress and well-being scores, as it was shown in a series of confirmatory factor analyses. The emotion regulation difficulties construct did not overlap with the psychological distress construct and the well-being one, suggesting that the DERS-8 scores could serve as an independent statistical predictor of other negative and positive mental health outcomes.
4.3. Predictive Ability of the DERS-8 Scores
We conducted two series of regression analyses and noted that emotion regulation difficulties (controlling for other demographic variables) were significant predictors of psychological distress (i.e., anxiety and depression symptoms) and well-being scores. Our research data supported the idea that these difficulties could be associated with both negative and positive mental health outcomes, suggesting that targeting emotion regulation difficulties might be beneficial for decreasing mental health burden and improving well-being. These difficulties were somewhat more strongly associated with psychological distress than with well-being, indicating a specific pattern across these links.
Overall, our results support past evidence regarding strong positive correlations of emotion regulation difficulties, measured with the DERS-8 and its long forms, with anxiety and depressive symptoms (e.g., [
13,
40]). We deem that the assessment of emotion-related constructs should include the perspective of the two continua model of mental health [
41], with its mental illness and mental well-being dimensions. In such cases, both negative and positive mental health outcomes are treated as potential correlates of the assessed constructs. In our study, taking into account both strong positive and negative correlations of emotion regulation difficulties with anxiety and depression symptoms and well-being scores, respectively, DERS-8 scores might serve as a potential transdiagnostic risk factor for common psychopathologies and poor well-being. However, causality should be determined in prospective studies.
4.4. Demographic Differences in Emotion Regulation Difficulties
Our study revealed several demographic patterns in emotion regulation difficulties. Females reported greater struggles with managing negative emotions compared to males, supporting previous empirical findings that emotional challenges may be more pronounced in females [
42,
43]. However, the effect size of these gender differences was small, which is consistent with the previous findings [
44].
In a series of ANCOVAs devoted to the demographic differences analysis, age was a significant covariate. Further exploration of the role of age in emotion regulation difficulties allowed us to note that difficulty regulating emotions was more prevalent among younger individuals than in the older ones in our data-set. These results are consistent with earlier research, suggesting that aging is associated with more efficient and adaptive emotion regulation due to the accumulation of life experience [
45,
46]. Our results indicate that younger individuals are at risk of psychopathology development, therefore assessing emotion regulation difficulties, which serve as a risk factor for a wide range of psychopathologies [
47,
48,
49], is particularly relevant for this group.
We were also interested in discovering whether education and relationship status categories (as less studied demographic variables in the emotion regulation field) differentiated difficulties with emotion regulation. We found that people without a university degree experienced slightly more difficulties in emotion regulation, but the effect size of these differences was negligible. The relationship status did not differentiate the DERS-8 scores.
To date, to the best of our knowledge, there are no studies on the demographic differences in DERS-8 scores, therefore, we cannot contrast our results with the previous ones. However, based on the obtained results and the past work on the full DERS (e.g., [
44]), we may conclude that age and gender seem to be the most relevant demographic factors, which should be taken into account while studying challenges in emotion regulation.
4.5. Norms and Their Interpretation and Other Practical Implications
Based on our data-set, we calculated Polish norms of the DERS-8 for the total sample and two age groups (aged 18–29 and 30–73 years old). The percentile rank norms were computed using a Bayesian approach, with 90% and 95% credible intervals for percentile rank scores. To facilitate the interpretation of the DERS-8 scores, we proposed to classify levels of emotion regulation difficulties based on the following categories of percentile rank norms [
50]: low levels (percentile ranks of ≤15), average levels (percentile ranks from 16 to 84), and high levels (percentile ranks of ≥85). Overall, a total DERS-8 score of ≥32 suggested high levels of emotion regulation difficulties in the total sample. We recommend using age-specific cut-off scores for high levels of these difficulties, with a total DERS-8 score of ≥33 in younger adults aged 18–29 and a total DERS-8 score of ≥29 in older adults aged 30–73. We would like to underline that these cut-off scores were calculated based on the current Polish sample and, therefore, may not generalize to other cultures.
The growing pace of life, along with specific research conditions, frequently requires researchers to use increasingly shorter tools, resulting in a greater demand for such measures [
21]. The concise design of the DERS-8 makes the assessment of difficulties in emotion regulation more practical and accessible in diverse settings. For instance, given its reduced number of items, DERS-8 is a good measure for quick screenings in general and clinical populations.
The development and implementation of interventions targeting emotion regulation in children and adults requires the use of well-operationalized measures of emotion regulation, with the DERS being a popular measure of interest [
11]. In the educational context, following the ideas that emotion regulation difficulties are positively related to academic burnout [
51] and student engagement and relations with peers and teachers [
52], we believe that the DERS-8 can be considered a good measure for quick screening of emotion regulation difficulties among students. In Poland, university students experienced high levels of anxiety and depression symptoms [
53]; therefore, screening assessments of emotion regulation difficulties and the development of psychological support programs targeting psychological distress and emotion regulation abilities seem to be pertinent. With the brevity of the DERS-8, such monitoring is very accessible.
Additionally, the DERS-8 supports long-term research aimed at targeted interventions for older adults [
19]. Moreover, the DERS-8 is also well-suited for studies requiring the tracking of emotion regulation difficulties over time or simultaneous evaluation of many constructs.
4.6. Limitations
This study has several limitations. First, its cross-sectional design does not allow for determining whether emotion regulation difficulties lead to mental health issues or vice versa, highlighting the need for further investigation of causality through longitudinal research. Secondly, our sample was not fully representative of the structure of the entire Polish population (e.g., the presence of gender imbalance). Also, participants choose to engage in psychological studies that align with their personal needs and traits, potentially introducing an unintentional self-selection bias [
54]. Additionally, online recruitment could have excluded individuals with limited Internet access, potentially leading to underrepresentation of certain groups (e.g., older individuals and people with limited Internet access). Thirdly, the small number of non-binary participants limited the ability to explore gender-based differences fully between females, males, and non-binary individuals, as well as to conduct measurement invariance across these three gender groups. Finally, by design, this was not a clinical study; therefore, we did not control participants’ clinical diagnoses, if there were any. Our study focused on a non-clinical adult sample, offering a foundation for future research involving more diverse groups, such as adolescents and individuals with various clinical diagnoses.
4.7. Future Directions
Several areas should be explored in future research on the DERS-8. First, while the DERS-8 primarily focuses on emotion regulation difficulties related to negative emotions, as the items begin with “When I am upset” [
18], it is relevant to develop a short tool that also assesses the difficulties in regulation of positive emotions [
55,
56]. Secondly, the DERS-8 was created to study both adults and adolescents [
18]; however, this study focused solely on adults. Consequently, future research should include adolescent populations to assess the scale’s validity and applicability across age groups. We also feel that there is an urge to study emotion-related variables in people with genders other than binary ones (i.e., female and male) to increase their visibility in the research and practice of healthcare [
57,
58]. Finally, as this study did not include clinical samples, future research should examine the DERS-8 among individuals with clinical diagnoses to evaluate its relevance and utility in clinical settings (e.g., [
13]).
5. Conclusions
The DERS-8 has demonstrated strong psychometric properties in an adult Polish sample. The Polish DERS-8 was characterized by the theoretically informed one-factor structure, which was invariant across several demographic categories (i.e., gender, age, education, and relationship status) and different levels of mental health outcomes. This indicates that DERS-8 scores can be collated across these groups pertinently. A good level of internal consistency reliability and strong convergent and divergent validity further supported the good psychometric performance of the scale. Moreover, emotion regulation difficulties, as measured with the DERS-8, were statistically set apart from the current level of one’s psychological distress, indicating that these constructs were theoretically and empirically distinguishable. As such, DERS-8 scores were strong predictors of anxiety and depression symptoms and well-being. As we calculated the current Polish norms for the freely available DERS-8, we believe that our study contributes to the clinical practice well, creating opportunities for the efficient prevention of emotion-based psychopathology among Polish adults.