
1. Introduction
Sport supplements, defined as “a food, food component, nutrient, or non-food compound that is purposefully ingested in addition to the habitually consumed diet with the aim of achieving a specific health and/or performance benefit” [1], are permitted by sport organizations [2], and widely used by athletes [3,4]. Athletes use sport supplements for a variety of reasons, including energy provision, health maintenance, management of nutrient deficiencies, recovery from injury, and performance enhancement [1,5,6,7,8].
The use of sport supplements has been linked with doping (i.e., the use of banned substances and methods). A meta-analysis showed that athletes who used sport supplements were 2.74 times more likely to dope and reported greater intentions and more favorable attitudes to dope than non-users [9]. Cross-sectional studies typically find that doping prevalence [10,11,12] and willingness [7] are higher among athletes who identify as supplement users than non-users. However, only a small fraction of athletes who use sport supplements also use doping substances and methods [11,13,14]. For instance, Hurst et al. (2023) [9] reported that 86.3% of those who used sport supplements did not dope. Thus, while sport supplements may increase the likelihood of an athlete doping, only a small proportion of sport supplement users go on to dope. This funneling effect has encouraged researchers to search for reasons why some athletes progress from using sport supplements to doping substances and methods.
The gateway hypothesis [15] has been used to explain the supplement–doping relationship. This hypothesis, first developed to explain recreational drug use, proposes a sequential progression from the use of “soft” drugs, such as tobacco or alcohol, to the use of “hard” drugs, such as marijuana and cocaine [15]. In the context of doping, athletes who use permitted substances, such as sport supplements, might be expected to progress to using prohibited substances, such as steroids and stimulants [10]. In line with this hypothesis, a retrospective study of students found that the use of protein preceded the use of creatine, which, in turn, preceded the use of steroids, which were used by 5.8% of the sample [16].
The gateway hypothesis considers the development of beliefs that the consumption of substances, including sport supplements, benefits athletic performance. In support of this notion, a qualitative study of elite cyclists reported that if athletes took a substance (sport supplement) in a race and won, they would take that substance in every race thereafter [17]. Therefore, the development of strong beliefs about the effectiveness of performance-enhancing substances could be a mechanism that leads users of supplements to become users of doping substances. Indeed, beliefs about the effectiveness of sport supplements may create beliefs that prohibited substances are more effective for performance enhancement, thereby placing such athletes at increased risk for doping [18].
Qualitative research reveals that athletes who believe sport supplements are necessary for success have more positive attitudes towards doping [17,19]. Cross-sectional research suggests that sport supplement users hold stronger beliefs that doping is effective and are more likely to use doping compared to sport supplement non-users, leading to speculation that supplement users attribute improvements in performance to the supplements themselves [10]. In support of this speculation, studies that measured beliefs about the effectiveness of sport supplements have consistently found that supplement users hold stronger beliefs than non-users [18,20,21,22]. These studies also showed that supplement use was indirectly related to doping attitudes and doping likelihood via sport supplement beliefs [20,21,22]. However, to date, no study has confirmed that this indirect relationship extends to the use of doping substances. The present study therefore tested whether supplement use was related to doping use via supplement beliefs.
Hundreds of different supplements are available to athletes and can be categorized into various types based on their purpose [3,23]. For example, an athlete can take medical supplements to overcome illness and injuries, such as iron and calcium, and take performance supplements, such as creatine and sodium bicarbonate, to improve their performance. The Australian Institute of Sport’s (2019) Sports Supplement Framework [23] distinguishes between groups of sport supplements, which are categorized depending on support for their scientific evidence. Group A supplements have shown strong scientific evidence of their effectiveness in improving sport performance and are separated into sport food supplements (e.g., sports drinks, protein shakes), medical supplements (e.g., iron, calcium), and performance supplements (e.g., caffeine, creatine). Group B supplements require further evidence and include sport supplements such as zinc, amino acids, and carnitine. Group C consists of supplements that have shown no scientific evidence that supported their use for sport performance and includes magnesium, vitamin E, and beta-hydroxy-beta-methyl butyrate. Finally, Group D sport supplements include those that are prohibited or have a high risk of being contaminated with a prohibited substance.
Importantly, while categories of supplements exist, most studies examining the supplement–doping relationship have simply asked participants a single-item question (i.e., yes or no) concerning whether or not they use/used sport supplements [9]. A few studies have adopted a differentiated approach to assess sport supplement use. First, Hildebrandt and colleagues found that the use of steroids by high school students (only 40% engaged in competitive sport) was associated with the use of muscle-building supplements and weight–fat loss supplements but not health–well-being supplements [24]. Moreover, those using muscle-building supplements (but not well-being supplements or weight–fat loss supplements) were more likely to dope due to the belief that the supplements are effective. Second, Hurst and colleagues found that users of sport food/drink supplements (e.g., protein powder), medical supplements (e.g., iron), and ergogenic supplements (e.g., creatine), but not superfood supplements (e.g., goji berries), held stronger sport supplement beliefs than non-users [21]. Moreover, users of medical and ergogenic supplements (but not sport foods and superfoods) also expressed more positive attitudes towards doping than non-users of these supplements. Finally, the stronger pro-doping attitudes expressed by users of sport foods and medical and ergogenic supplements (but not superfoods) were mediated by their stronger beliefs about the effectiveness of sport supplements. Taken together, these findings suggest the possibility that athletes develop beliefs that certain sport supplements are beneficial for performance and these beliefs foster more positive attitudes towards doping in some athletes. Nonetheless, pro-doping attitudes do not necessarily lead to doping behavior [25]. Accordingly, research is needed to assess the role of beliefs in the relationship between supplement use and actual doping behavior. The present study examined this possibility by assessing the use of supplements based on an established framework developed by a major sporting organization.
The aim of our study was to examine the relationship between the use of sport supplements and doping in competitive athletes. We had two specific purposes. The first was to determine the use of sport supplements [23] and doping substances [26] in athletes. We hypothesized a high prevalence of supplement use and a low prevalence of doping use. The second was to examine direct and indirect (via sport supplement beliefs and/or doping likelihood) effects of sport supplement use on doping use. We hypothesized that supplement use and supplement beliefs would be positively associated with doping likelihood and doping use.
3. Results
Details of the habitual use of sport supplements are summarized in Table 1. The most commonly used supplements in each category were sports drinks (77%) among sport foods in Group A, multivitamins (55%) among medical supplements in Group A, caffeine (66%) among performance supplements in Group A, and food polyphenols (49%) in Group B. Most athletes (96%, n = 332) reported using one or more of the 23 sport supplements. AIS Group A supplements were used by 96% (n = 331) of the athletes, which, broken down by category, indicated that 90% (n = 310) used sport food supplements, 64% (n = 222) used medical supplements, and 72% (n = 250) used performance supplements. AIS Group B supplements (i.e., category “other” supplements), were used by 66% (n = 227) of the athletes. Furthermore, 11% (n = 37) used supplements from one category, 18% (n = 61) used two categories, 25% (n = 86) used three categories, and 43% (n = 148) used four categories of sport supplements.
In terms of the use of doping, very few athletes (4%, n = 14) reported using one or more of the six classes of doping substances and methods. Moreover, 14 out of the 14 athletes (100%) who used a doping substance used at least one AIS sport supplement, whereas 318 out of the 331 athletes (96%) who did not use a doping substance used at least one AIS sport supplement.
Table 2 presents the descriptive statistics and correlations among variables. The athletes used many sport supplements, believed supplements were effective for sport performance, were unlikely to use doping substances in hypothetical situations, and used few, if any, doping substances and methods. The Pearson correlations indicated that sport supplement use was positively related to sport supplement beliefs and doping use, sport supplement beliefs were positively related to doping likelihood, and the doping likelihood was positively related to doping use.
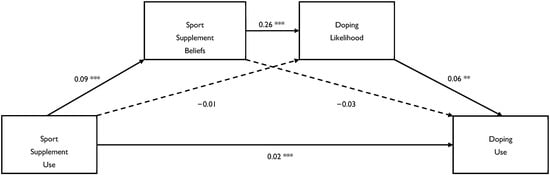
The PROCESS 4.2 [31] model concerning the direct effect and indirect effects (via beliefs and/or likelihood) of sport supplement use on doping use are depicted in Figure 1. It shows that sport supplement use had a direct effect on doping use, 0.021, 95% CI = 0.009, 0.034, t = 3.33, p < 0.001, and an indirect effect on doping use via supplement beliefs and doping likelihood, CSIE = 0.011, 95% CI = 0.003, 0.023, p < 0.05. In other words, the increased frequency of doping use was directly explained by the increased frequency of consuming sport supplements and indirectly explained by stronger beliefs about supplements and a greater likelihood of doping in hypothetical situations.
4. Discussion
Grounded in the gateway hypothesis, our study sought to determine the prevalence of supplementation and doping, examine the relationship between the use of sport supplements and the use of doping substances, and investigate supplement beliefs and doping likelihood as mechanisms underlying the supplement–doping relationship.
Our first study purpose was to determine the frequency of using sport supplements [23] and doping substances/methods [26]. The list of supplements was taken from Groups A and B of the AIS’s Sports Supplement Framework [23]. Among the 23 sport supplements, prevalence ranged from a low of 7% (bicarbonate) to a high of 77% (sports drink), with an average of 32%. We found that nearly all athletes (96%) used at least one sport supplement in the last six months or previously, and that most athletes used multiple supplements, with athletes consuming seven different classes of supplements on average. Although differences in participants, timeframes, and definitions present difficulties comparing studies, our prevalence rate is consistent with, albeit at the high end of, previous estimates of 40–100% [3]. The current prevalence of supplementation by athletes is similar to a recent study that examined the use of a range of supplements and reported that 97% of athletes used at least one supplement in the last month [7]. Moreover, we found that athletes used a variety of supplements from the three Group A subcategories of supplements that the AIS deems to possess evidence to support their use in sport (sport foods, medical supplements, performance supplements) as well as, albeit to a lesser extent, supplements from the Group B subcategories of supplements, which the AIS stated were currently lacking evidence to support their use by athletes. In contrast, we found that very few athletes reported using one or more of the six classes of doping substances and methods [26]. The prevalence of reported doping in the current sample of athletes (4%) exceeds that typically reported in WADA’s annual anti-doping rule violation database, where the prevalence is less than 1% [32]. However, the current prevalence rate is broadly in line with the majority of past research, with most studies reporting rates of less than 5% [33]. Taken together, and in agreement with past research (e.g., [9]), our findings reveal that most doping users use sport supplements but few sport supplement users also use doping substances.
Our second study purpose was to examine the direct and indirect (via sport supplement beliefs and/or doping likelihood) effects of sport supplement use on doping use. Extending past research [20,21,22], we found that sport supplement use was indirectly related to doping use via sport supplement beliefs and doping likelihood (Figure 1). These replications implicate beliefs as an intermediary factor in supplement–doping relationships and suggest that the perceived performance benefits of using chemically active substances may permit athletes to view the use of doping substances as similarly effective, which may foster positive attitudes towards their use. Moreover, we found that sport supplement use was indirectly related to doping use via a combination of both sport supplement beliefs and doping likelihood, suggesting that athletes who use sport supplements are more likely to use doping substances when they believe that the consumption of sport supplements is likely to enhance their performance and when they are tempted to use prohibited substances in specific situations that they might encounter, such as those associated with reduced personal responsibility and increased rewards. Accordingly, both of these personal factors (i.e., beliefs and likelihood of being tempted) may increase an athlete’s risk of using doping substances.
In sum, our findings broadly replicate previous research [20,21,22,24], and, at least at first glance, partially support the gateway hypothesis (cf. [15]). Specifically, athletes who used more sport supplements were more likely to use more doping substances and methods. As specified by the gateway hypothesis, athletes’ consumption of permitted substances represents the opening of a gate to the consumption of prohibited substances. Despite all doping users also being supplement users, most supplement users were not users of doping substances. It could therefore be argued that the current data fail to offer clear support for the gateway hypothesis. This reasoning underscores the weaknesses associated with using a simple binary yes/no question about supplement use that is most commonly used in previous research [9]) and instead emphasizes the benefits of assessing supplement use in more detail, such as the total number of supplements used. Finally, the current findings argue for the need to look for potential moderators of the supplement–doping relationship, such as the demands of the sport, time of the season, and motivation.
Source link
Philip Hurst www.mdpi.com